
Only 3.4% of Worship Leaders rate their mental health as excellent compared to 29% of U.S. adults, and 9 in 10 get no help at all.
Only 3.4% of Worship Leaders rate their mental health as excellent compared to 29% of U.S. adults, itself a historic low. At the same time, 87% of Worship Leaders do not meet regularly with either a mental health professional or a spiritual director. The youngest Worship Leaders (18-29)—the very same generation driving a national surge in therapy—are the least likely to be getting help.
These are among the findings of the largest research survey of Worship Leaders ever conducted in North America: more than 3,300 respondents across a variety of denominations, traditions, and regions. The picture that emerges is not one of crisis. It is something quieter and, in some ways, harder to address: a population high in purpose, moderate in distress, and remarkably low in professional or structured care.
Harvard professor Tyler VanderWeele’s finding that regular religious attendance is associated with significantly lower risk of “deaths of despair” made national headlines when he called church attendance a “Miracle Drug” in USA Today. The implications were inspiring. But they raise an unavoidable question: what about those at the front? A growing body of evidence on clergy burnout—including Barna research showing that 65% of pastors report loneliness and isolation—suggests that the view from the platform may differ significantly from that in the pews.
In what follows, we explore several key findings in depth before highlighting areas for further investigation.
In our survey, Worship Leaders were asked to report on their mental health in a manner similar to larger, more wide-reaching national surveys. These comparisons are not exact (our survey, at times, used slightly different instruments than national datasets), but the patterns they reveal are striking nevertheless.
The Excellence Enigma
Only 3.4% of worship leaders in our sample rate their mental health as excellent. In Gallup’s most recent data, 29% of U.S. adults say the same, a figure that dropped below 30% for the first time in 2025, down from a pre-pandemic average of roughly 43%. By either benchmark, the gap is striking. Worship leaders are roughly 8.5 times less likely than the general public to place themselves at the top of the self-rated mental health scale.
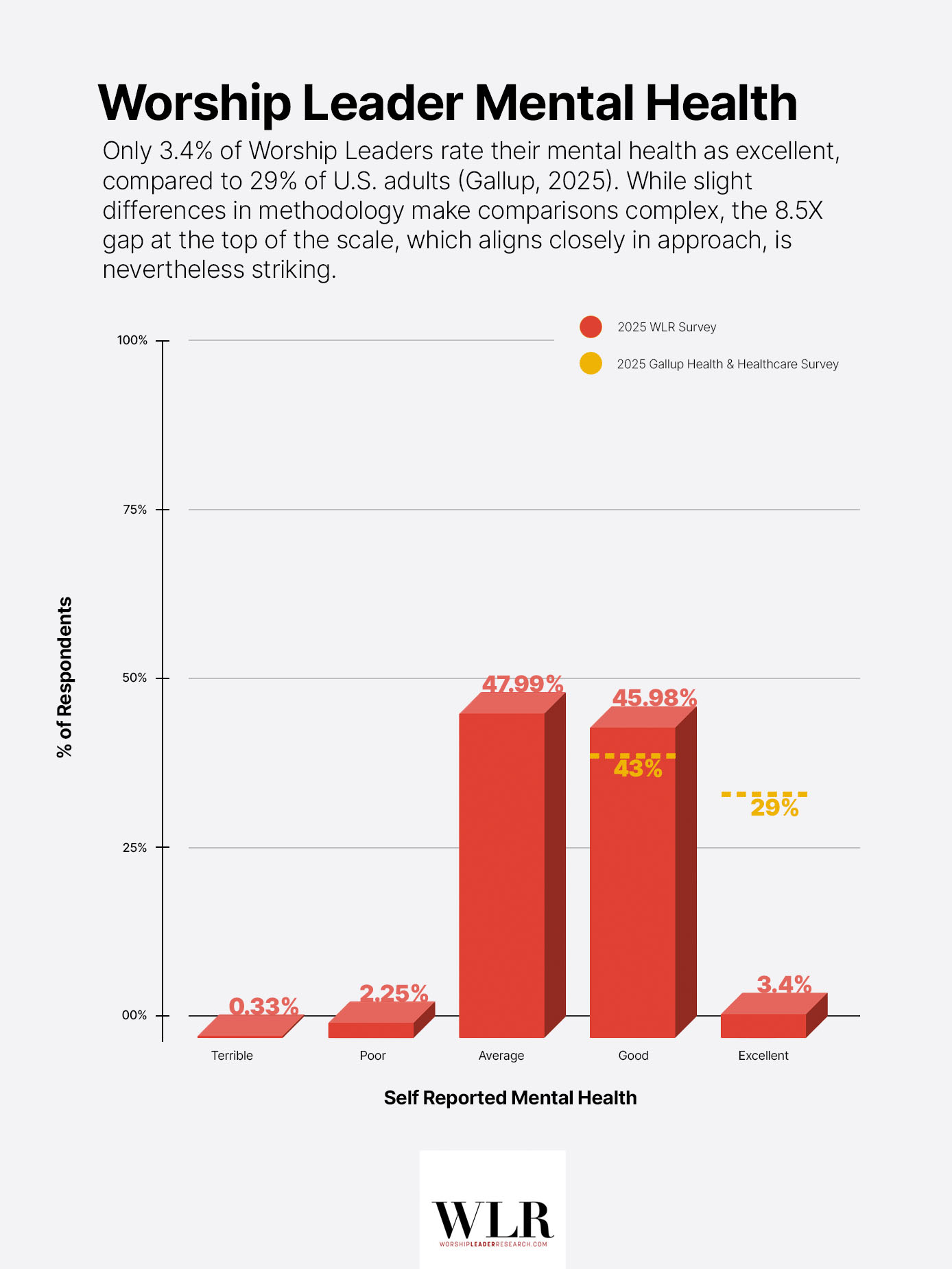
Gallup’s combined “excellent” and “good” rating captures 72% of U.S. adults, itself a record low. Among Worship Leaders, the equivalent figure is 49.4%: a gap of more than 22 points. Our scale includes five options (excellent, good, average, poor, terrible) while Gallup uses four (excellent, good, only fair, poor). Even so, the direction and magnitude of the gap are difficult to dismiss.
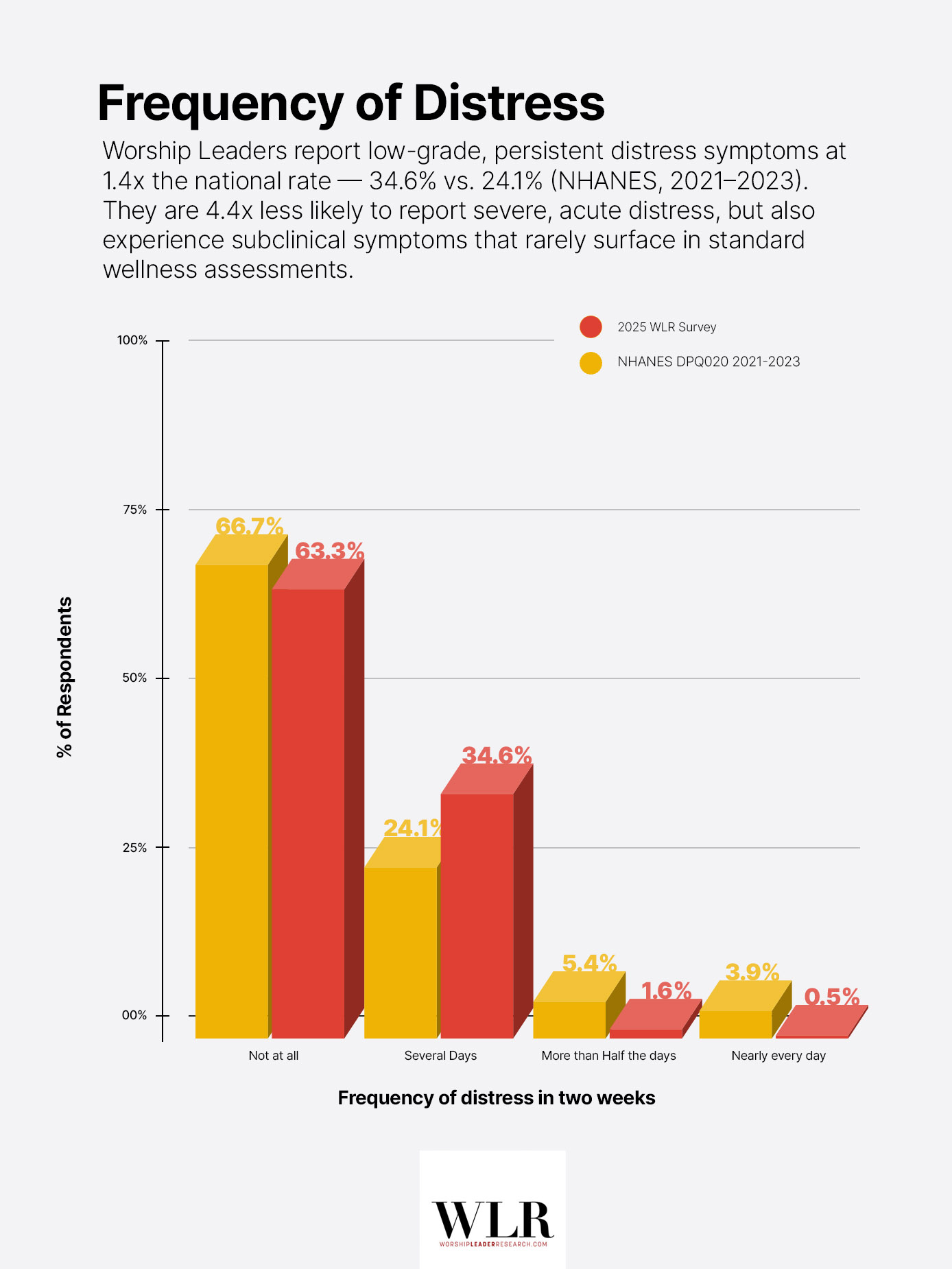
With that said, the lower end of the scale tells a more encouraging story. Survey respondents were roughly 4.4 times less likely than the general population to report severe or acute distress symptoms. Only 2.1% of Worship Leaders report frequent symptoms (more than half the days or nearly every day), compared to 9.2% nationally on the closest comparable NHANES item (NHANES DPQ020, August 2021–2023). By this measure, Worship Leaders appear to be avoiding the most acute distress in a meaningful way.
But the most notable finding may, in fact, be hiding in plain sight: approximately 34.6% of respondents report distress symptoms for several days over two weeks, compared to 24.1% (NHANES)—1.4 times the national average. These are subclinical, low-grade symptoms: persistent enough to affect daily experience, but unlikely to surface in standard wellness assessments.
Worship Leaders are, as a group, not in crisis. But they are certainly not thriving.
The Purpose Paradox
A sense of purpose at work is often considered one of the most robust predictors of psychological well-being in the research literature. A meta-analysis of 146 independent samples found that meaningful work was strongly associated with life satisfaction, job satisfaction, positive affect, and more. By this measure, Worship Leaders should be in an enviable position. In our sample, 78.6% report experiencing a sense of purpose or fulfillment in their role more than half the days or nearly every day. For comparison, a 2025 Gallup/Stand Together study of 4,475 U.S. working adults found that only 18% report strong purpose in their work, making Worship Leaders more than four times as likely to experience frequent purpose compared to the average American worker.
Yet this purpose does not seem to be producing the predicted outcome.
Only 44.3% of respondents report frequent joy or contentment in the role, 34 percentage points below their reported sense of purpose. This gap is worth underscoring. It suggests that while many Worship Leaders experience their work as deeply meaningful, some do not find it consistently enjoyable on a day-to-day basis.
Something appears to be hindering the benefits of this well of purpose.

Sources of Distress
Of course, if we want to know what that something might be, we can turn to respondents themselves. In our survey, Worship Leaders were asked to identify the greatest sources of mental health challenges in their role. Three sources were selected at notably higher rates than the rest.


At first glance, these top-line results are broadly consistent with what existing literature on clergy wellbeing would predict. The Duke Clergy Health Initiative, for instance, identified job stress, navigating competing demands, and guilt about not doing enough as top predictors of depression among pastors.
One additional finding provides useful context. Work satisfaction among Worship Leaders is remarkably stable across both age and symptom frequency. The proportion reporting “very satisfied” hovers between 36% and 40% from ages 18 through 59, with no meaningful variation. Even among respondents reporting frequent distress symptoms, a majority (69.0%) describe themselves as at least “moderately satisfied.” Worship Leaders experiencing significant distress do not, on the whole, report dissatisfaction with the work itself.
Leader, Heal Thyself
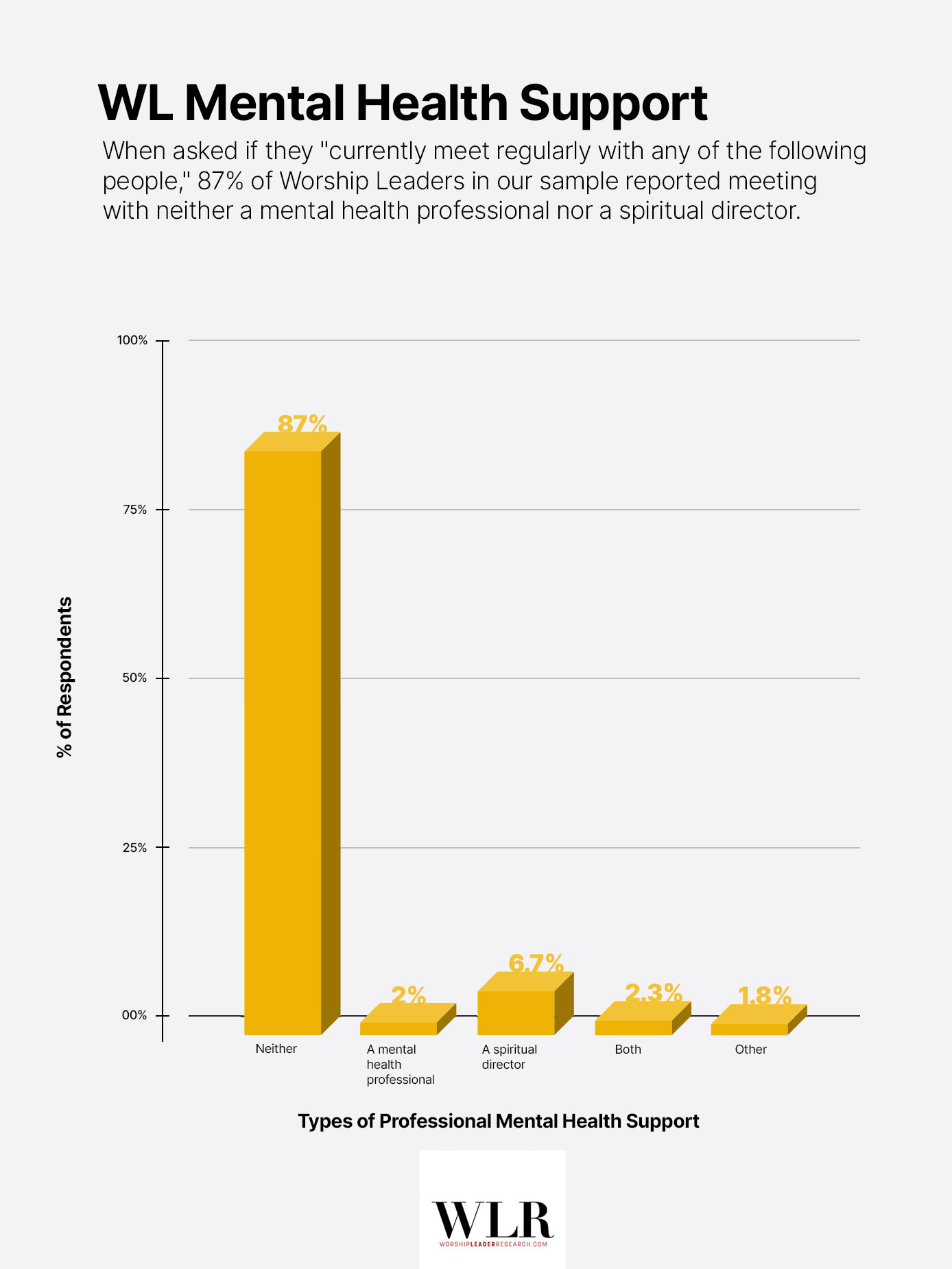
87% of Worship Leaders in our sample do not meet regularly with either a mental health professional or a spiritual director.
Were we to restrict the data to meetings with mental health professionals alone (excluding spiritual directors), the number rises to approximately 95.7%. In a nation where roughly 24% of U.S. adults report seeing a mental health professional in the past year, Worship Leaders appear to be accessing professional support at a fraction of the national rate.
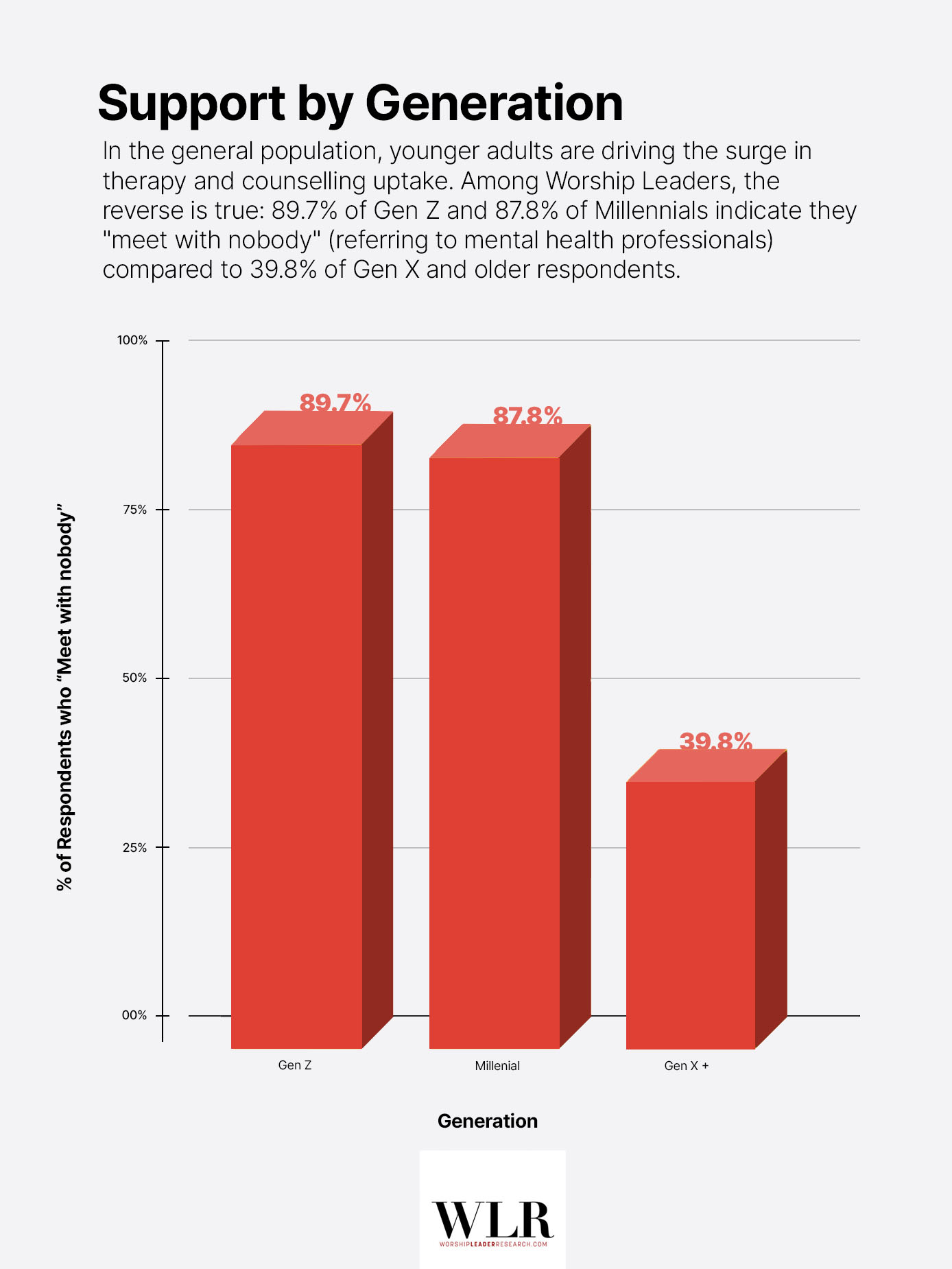
This gap is not uniform across ages. Among Gen Z, 89.7% of Worship Leaders meet with neither a professional nor a spiritual director, similarly to Millenials at 87.8%. Among participants belonging to Gen X and beyond, that number drops to 39.8%.
An Inverted Generation
The role of age deserves particular attention, if only because it runs directly counter to one of the most well-documented trends in national mental health data. In the general population, younger adults are driving the surge in therapy and counselling uptake. Gallup’s most recent data shows that 36% of Gen Z adults and 29% of millennials report having seen a mental health professional in the past year, compared to just 14% of baby boomers and 7% of the Silent Generation. Among Worship Leaders, the reverse is true. The Gen Z cohort reports the highest rate of meeting with nobody—only 2 points higher than Milennials—even though they are the exact demographic most likely to seek therapy in national studies.
This is compounded by the fact that younger Worship Leaders also report feeling less supported by their congregations than their older peers. Among 18–29 year-olds, 43.4% report feeling high levels of congregational support (selecting “quite a bit” or “a lot”). That figure rises to 75.7% among those 60–69, though it is worth noting that many have aged out of the position by that stage of life, as reflected in a small sample size beyond age 50. Nevertheless, it seems younger Worship Leaders are, at once, less likely to seek outside help and less likely to feel supported from within the walls of the church.
Self-Care Without Infrastructure
It would be inaccurate to say Worship Leaders are doing nothing at all. When asked whether they engage in self-care practices, 86.7% say yes. The most commonly listed activities drawn from their responses are prayer, exercise, time in nature, hobbies, and reading scripture. But when asked how effective their self-care efforts are, 83.6% of those practicing self-care describe their efforts as only “moderately effective.” Just 15.1% say their practices are “very” or “extremely” effective.


Worship Leaders are, in other words, trying. What they are doing is largely informal, self-directed, and only moderately helpful, and infrastructure such as professional counselling or funded spiritual direction appears mostly absent from their experience.
A Point of Comparison
Our survey did not ask about medication use, insurance coverage, or financial barriers to care. It is plausible that some of the 87.1% are receiving pharmaceutical support through primary care without regular counselling. It is equally plausible that cost, stigma, or the structural expectations of ministry are barriers to more comprehensive support.
What it does suggest is that Worship Leaders exist in a support desert: high in purpose, moderate in distress, and remarkably low in professional or structured care. This is consistent with research on pastors more broadly. The Duke Clergy Health Initiative found that even among clergy with elevated symptoms, mental health service use remained well below what symptom levels would predict.
What We Still Don’t Know
Our data shows what the lived experience of Worship Leaders looks like. It cannot tell us why. But several questions demand attention.
Why are the youngest Worship Leaders the least likely to access support?
89.7% of 18–29-year-old Worship Leaders report meeting with no one about mental health, whether licensed therapists or spiritual directors. This is the exact demographic driving a national surge in therapy uptake, with 36% of Gen Z adults nationally reporting having seen a mental health professional in the past year. What is it about the ministry context that overrides this generational openness? Is it financial? Cultural? Structural? Whatever the explanation, the inversion is striking.
Why does the gender pattern reverse?
In every national dataset we are aware of, women report higher rates of distress symptoms than men, but among Worship Leaders in our study, men report a higher frequency of symptoms (3.1% vs. 0.9%).
In the youngest grouping (18-29), women self-report mental health 4 points higher than their male counterparts, and women (18-29) are also 7 points more likely to engage in self-care practices.
The question is whether the role’s relationship to gender could help explain this gap.
Research on male help-seeking has consistently found that men who endorse traditional masculine ideals such as stoicism, self-reliance, or emotional control are significantly more likely to delay or avoid seeking support, even in severe distress. Worship Leaders occupy a public role in which emotional and spiritual health are performed weekly. The intersection of masculine norms with the expectation of visible spiritual resilience may create a uniquely difficult environment for men to acknowledge their own mental health needs.
Do Worship Leaders become resilient or age out?
Mental health outcomes improve sharply after age 50 but so do several other important variables. Perceived congregational support increases from 43.4% at 18–29 to 75.7% at 60–69. Similarly, congregational pressures drop from 47.6% among 18–29 to 14.8% among 50–59, representing a dramatic shift. Yet the sample gets dramatically, almost unavoidably small, with 55 respondents aged 50–59 and only 37 at 60–69.
Is this a genuine shift? The result of accumulated wisdom, greater autonomy, and reduced pressure? Do churches that employ 18-29 year-olds in the role simply place different pressures on their team than those content with a 60-69 year-old? Or is it survivorship bias, with those most affected having already left the role? While we don’t have the answers, the question matters. If attrition is a significant factor, the flat mental health scores from 18–49 may not represent a stable population learning to cope. They may represent a shrinking one.
Is purpose without joy sustainable?
78.6% of Worship Leaders experience frequent purpose. Only 44.3% experience frequent joy. The 34-point gap raises a question about longevity. If purpose alone is sustaining Worship Leaders through their 20s, 30s, and 40s, with flat mental health and flat satisfaction scores across those decades, what happens when purpose itself begins to fray?
Conclusion
Every week, Worship Leaders stand at the front of what research suggests may be one of the most protective experiences in American life—one dubbed a “Miracle Cure” for mental health. They lead others into something that lowers the risk of depression, addiction, and death by despair. And yet a mere 3.4% describe their own mental health as excellent, a 34-point gap between the purpose they feel and the joy they experience, and an 87% chance they’ll meet with nobody about any of it.
The miracle drug, it turns out, does not appear to be quite as effective for the people dispensing it. The Worship Leaders are not (quite) alright. So what are we going to do about it?








{kind=link}
{kind=link}
{kind=link}
{kind=link}